Gum disease is one of the most common reasons for adult tooth loss, and it often starts with something easy to ignore: a little bleeding when you brush. The good news is that early periodontal disease is often reversible, but once bone support is lost, the stakes change fast.
The Short Answer: How Gum Disease Can Cause Tooth Loss
Gingivitis is the early stage of gum disease, and it is typically reversible with better plaque control and a professional cleaning. Periodontitis is the advanced stage, and it can cause permanent damage that raises the risk of tooth loss.
The core mechanism is infection-driven inflammation. Bacteria living in dental plaque biofilm trigger an immune response that damages the gums, the periodontal ligament, and the alveolar bone that holds teeth in place.
Tooth loss risk depends on severity, duration, and risk factors like smoking, tobacco use, and diabetes. Genetics, dry mouth, certain medications, stress, and hormonal changes can also shift the odds.
Gingivitis vs. Periodontitis: Why Stage Matters
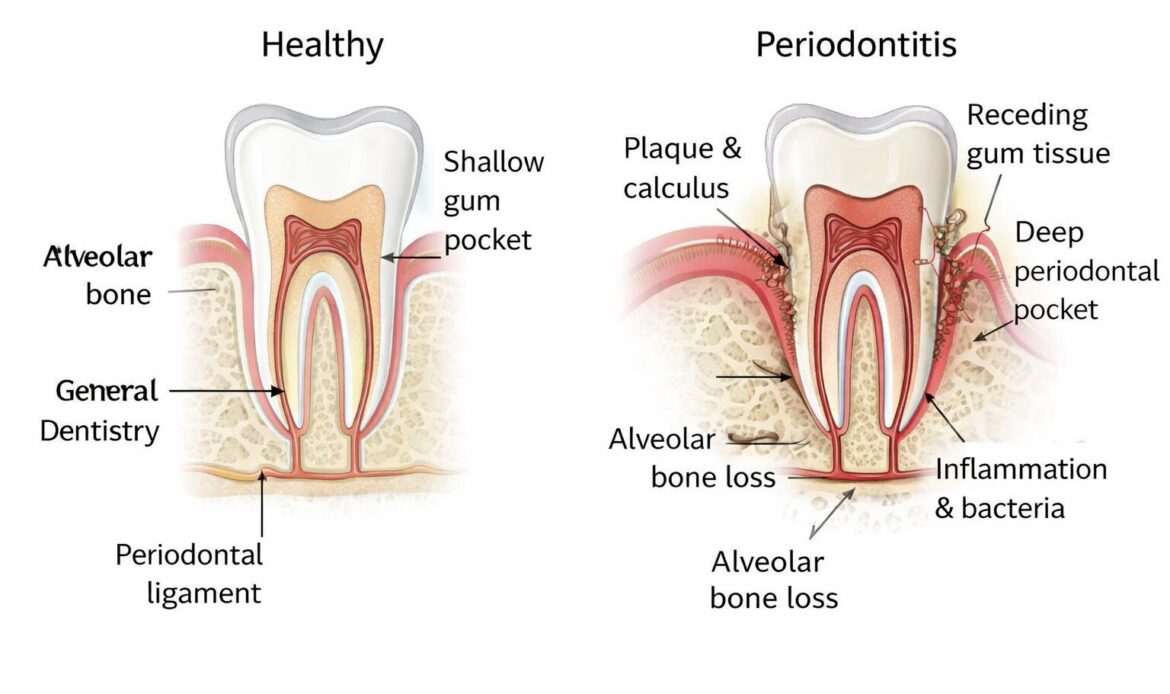
Gingivitis is plaque-related inflammation at the gumline without bone loss. Common signs include red, swollen gums, tender gums, and bleeding with brushing or flossing.
Periodontitis involves clinical attachment loss, periodontal pockets, and bone loss that can be seen clinically and on radiographs. As pocket depth increases, tooth mobility becomes more likely, and loose teeth can follow.
What “Tooth Loss” Looks Like Clinically
Periodontal breakdown usually looks gradual, not dramatic. It often progresses from gum recession and deeper pockets to tooth mobility, tooth shifting, bite changes, and then either spontaneous tooth loss or tooth extraction due to poor prognosis.
That’s different from sudden loss caused by injury or trauma. With periodontal disease, the tooth is often present but progressively less supported until normal chewing forces become destructive.
Step-by-Step: The Disease Process That Weakens Tooth Support
Step 1 is plaque biofilm buildup along the gumline. The bacteria in dental plaque biofilm release toxins and trigger inflammation.
Step 2 is calculus formation. Calculus, also called tartar, is hardened plaque that creates a rough surface where more biofilm sticks, especially near and under the gums.
Step 3 is pocketing and a bacterial shift. Periodontal pockets deepen, oxygen levels drop, and the biofilm tends to favor more aggressive bacteria, sustaining chronic infection and chronic inflammation.
Step 4 is loss of stability. As inflammation destroys the periodontal ligament and supporting bone, teeth lose attachment, and chewing forces accelerate mobility and damage.
Why Bone Loss Is the Turning Point
Alveolar bone resorption is the tipping point because bone is the foundation for tooth stability. Once bone loss occurs, the periodontal ligament has less structure to attach to, and tooth mobility becomes easier to trigger.
Bone resorption can be painless and easy to miss. Many people only notice a problem when they see gum recession, feel sensitivity, or realize their bite no longer fits the same way.
Why Home Care Alone May Stop Working
When pockets deepen, toothbrush bristles and floss often cannot reach subgingival plaque effectively. That means you can brush “well” and still leave a mature biofilm untouched below the gumline.
Professional debridement is designed to disrupt and remove plaque and calculus in areas you cannot access. That is why deep cleaning, not a new toothpaste, is often the turning point for controlling periodontitis.
Warning Signs, Risk Factors, and When to See a Dentist
Common symptoms include:
- Bleeding gums during brushing or flossing
- Bad breath or halitosis that keeps coming back
- Swollen gums or tender gums
- Gum recession or teeth that look “longer”
- Sensitivity, especially near the gum-line
- Pus or drainage, sometimes from a periodontal abscess
- Loose teeth, tooth mobility, or tooth shifting
- Bite changes or a new gap between teeth
Major risk factors include smoking and other tobacco use, diabetes (especially if poorly controlled), poor oral hygiene, genetics, dry mouth, and certain medications that reduce saliva or affect gum tissue. Hormonal changes can also matter, and pregnancy gingivitis is a classic example of gums becoming more reactive to plaque.
Seek urgent care if you notice a loose tooth, facial swelling, a suspected abscess, worsening pain, pus, or sudden bite changes. Those can signal active infection that needs prompt treatment, not watchful waiting.
Symptoms People Often Miss Until It’s Advanced
Bleeding during brushing or flossing is often dismissed as “normal,” but it is one of the clearest early signs of gingivitis. Healthy gums typically do not bleed with gentle, consistent cleaning.
Slow tooth shifting can be even easier to miss. If you’re suddenly trapping food in new spaces, noticing small gaps, or feeling that your teeth touch differently when you bite, periodontal breakdown is on the short list of causes.
How Dentists Diagnose Gum Disease Severity
Diagnosis is based on measurements and patterns, not guesswork. Dentists and hygienists use periodontal probing to measure pocket depth around each tooth and record bleeding on probing.
They also track clinical attachment loss, recession measurements, and areas of inflammation. Dental X-rays, also called radiographs, help assess bone loss patterns and can reveal calculus under the gum-line that cannot be seen directly.
If you want a clearer sense of what providers look for across different presentations, you can review the range of problems covered in these gum health evaluations and treatments: care options for different gum disease concerns.
Treatment Options to Help Prevent Tooth Loss
Early disease often responds well to a professional cleaning plus improved daily plaque removal. Risk-factor control matters here, especially smoking cessation, diabetes management, and addressing dry mouth.
Moderate to severe periodontitis commonly needs scaling and root planing, followed by periodontal maintenance visits on a tighter schedule. Clinicians sometimes use antibiotics in selected cases, but they are not a substitute for physically removing biofilm and calculus.
Advanced disease may require periodontal surgery, flap surgery, and in some cases guided tissue regeneration or bone grafting. If a tooth has severe mobility and poor remaining support, tooth extraction may be the healthiest option, followed by a plan to restore function with dental implants or bridges.
Non-Surgical Periodontal Therapy (First-Line)
Scaling and root planing, often called deep cleaning, removes plaque and tartar from root surfaces and periodontal pockets. The goal is to reduce inflammation, shrink pocket depth where possible, and make the root surface harder for biofilm to cling to.
A re-evaluation visit checks healing and remaining pocketing. Many patients with a history of periodontitis do best with periodontal maintenance every 3 to 4 months, because the biofilm matures faster in deeper sites.
Surgical and Regenerative Options (When Needed)
Flap surgery gives access to deep deposits and allows pocket reduction so home care can work again. In the right anatomy, that can slow progression and reduce the risk of future periodontal abscess episodes.
Clinicians can consider regenerative procedures for select defects. Bone grafting, membranes for guided tissue regeneration, and biologics may improve support in certain patterns of bone loss, but outcomes depend heavily on defect type and follow-through.
If tooth extraction becomes necessary, replacement timing matters for bone preservation and function. These two resources explain common implant decisions after losing a tooth: reasons some patients choose an implant for a missing tooth and what to know about implants after an extraction.
Prevention, Common Mistakes, and a Realistic Takeaway
Brush twice daily with fluoride toothpaste and clean between teeth every day. Routine dental visits matter because periodontal pockets and early bone loss can be hard to spot without periodontal probing and dental X-rays.
Control modifiable risks where you can. Quitting smoking, tightening diabetes control, addressing dry mouth, and reviewing medications with your clinician can reduce inflammation and improve healing.
Common mistakes keep periodontitis active:
- Waiting for pain before booking an exam
- Stopping flossing because gums bleed, instead of improving technique and consistency
- Skipping periodontal maintenance after treatment because “it feels better now”
- Assuming bad breath is only a stomach issue, not a gum infection issue
Gum disease is a leading cause of adult tooth loss, but it is not inevitable. Early detection, consistent biofilm control, and the right maintenance schedule often keep teeth stable for decades.
If you’re interested in how untreated gum problems may relate to whole-body health risks, this discussion is worth reading: why ignoring gum symptoms may affect more than your mouth.
Mini Case Example: From Bleeding Gums to a Loose Tooth
A common timeline looks like this: months of bleeding during brushing, then gum recession and persistent halitosis. Over years, periodontal pockets deepen, radiographs show bone loss, and one molar starts to feel “different” when chewing.
Earlier intervention points include a dental cleaning, improved interdental cleaning, and addressing smoking or diabetes. Later intervention often means scaling and root planing, periodontal maintenance every few months, and sometimes surgery if pocket depth stays high.
Gum recession is also a frequent clue that prompts people to finally ask questions. If recession is part of what you’re seeing, this breakdown of causes and treatment options can help you connect the dots: what drives gum recession and how it’s treated.
At-Home Routine That Actually Helps
Focus on removing plaque where gum disease starts: along the gumline and between teeth. A solid routine is simple, but it has to be consistent.
- Brush for two minutes, aiming bristles slightly toward the gumline to disrupt biofilm
- Use floss or interdental brushes daily, choosing the size that actually contacts tooth surfaces
- Consider a water flosser as an adjunct, especially around bridges, implants, or tight orthodontic areas
- Use antimicrobial mouthwash short-term if recommended, but don’t treat it like a “quick fix” for tartar or deep pockets
If you’re unsure whether you’re dealing with gingivitis or periodontitis, you can review this evidence-based overview of periodontal disease from the National Institute of Dental and Craniofacial Research. Pair that general guidance with an exam, because clinicians can’t accurately diagnose pocket depth and attachment loss at home.
FAQ: Gum Disease and Tooth Loss
Can gum disease cause tooth loss?
Yes. Untreated periodontitis can destroy the gum and bone support around teeth, leading to tooth mobility, loose teeth, and eventual tooth loss or tooth extraction.
How long does it take for gum disease to cause tooth loss?
It varies. Gingivitis can progress to periodontitis over time, and bone loss often happens gradually over months to years depending on risk factors like smoking, diabetes control, genetics, and how consistently a person removes plaque.
Can loose teeth from gum disease be saved?
Sometimes. With prompt periodontal treatment, clinicians can control inflammation and improve stability, but advanced clinical attachment loss and severe alveolar bone loss can limit how much support clinicians can regain.
What are the first signs of gum disease?
Early signs commonly include bleeding when brushing or flossing, red or swollen gums, and persistent bad breath. Tender gums and mild gum-line swelling are also common in gingivitis.
How do I prevent gum disease from getting worse?
Remove plaque daily with brushing and interdental cleaning, keep regular dental visits, and follow periodontal maintenance if you’ve treated periodontitis. Address risk factors such as tobacco use, control diabetes, manage dry mouth, and review medication-related mouth dryness with your dental and medical team.